
Research
A Compelling Overview
One of the areas in which chiropractic has faced the most challenge is in what is called “evidence-based” health care. This has emerged out of the desire on the part of insurance companies to reduce their costs and increase their profits. This is most easily done by first refusing to cover certain treatments, and then by reducing the amount they pay for a treatment. The fact that over the last hundred years chiropractic has survived a focused attack from the American Medical Association is unimportant to insurance companies. The fact that chiropractors have survived and thrived because of our patients’ efforts to make and keep chiropractic legal and legitimate is unimportant to insurance companies. The fact that over 30,000 jail terms were served by chiropractors for “practicing medicine without a license” in states that were unwilling to license us, because those chiropractors refused to stop doing what they knew was right for their patients, is unimportant to insurance companies. The fact that there are clinical, though anecdotal, cases of chiropractic helping with every health condition known to man, has little to do with gaining credibility.
Despite the challenges, there is a fast-growing body of research on chiropractic. Much is from overseas from countries like Britain, Australia and Canada, where the health care system is public, and public access to records makes research easier. Some is from the USA despite the fact that research here is mostly funded by pharmaceutical and medical equipment companies that arguably have an active interest in preventing research on an inexpensive, natural, noninvasive treatment. To be fair, the great differences in the way chiropractic is practiced, and the fact that almost every state outlines a different scope of practice for chiropractors, makes research more difficult. Since we cannot agree as a profession on what chiropractic is, it is difficult to design an effective research strategy.
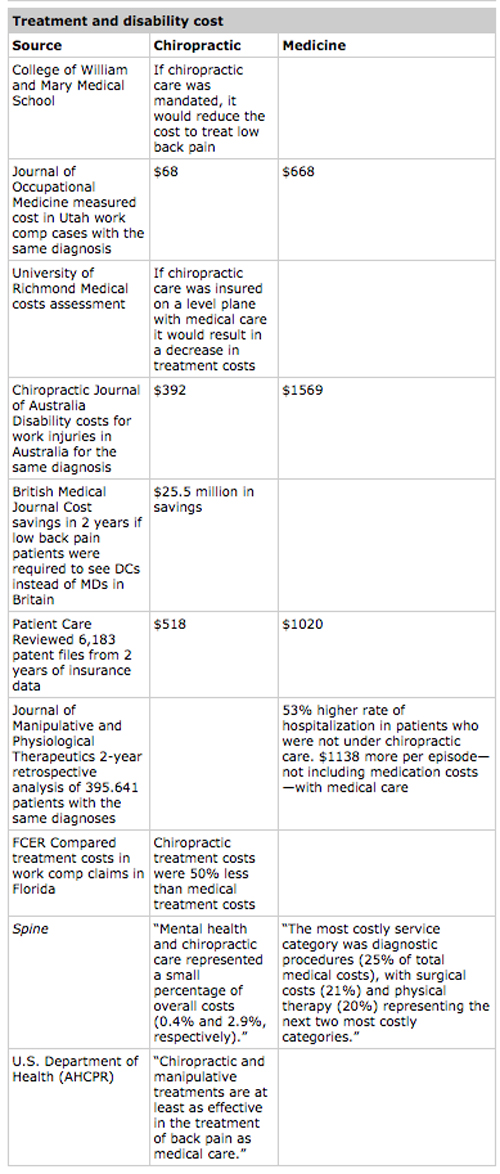
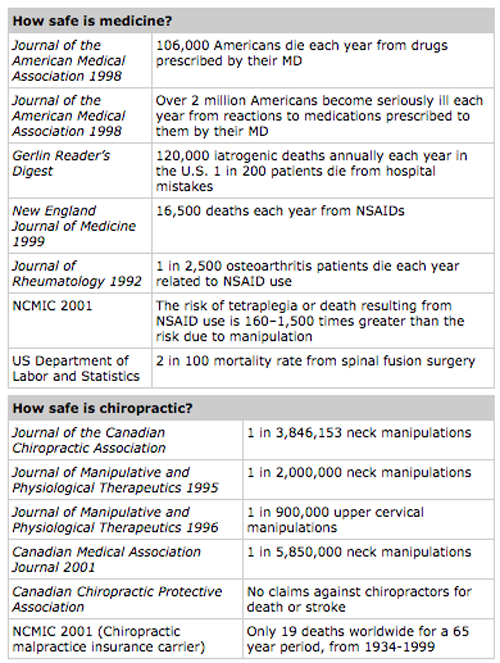
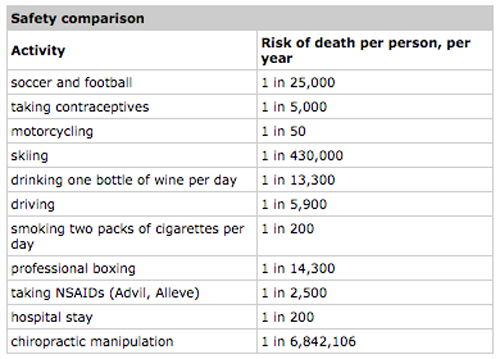
Below are listed some of the most compelling studies on chiropractic and their results. They provide a perspective on the cost, safety and effectiveness of chiropractic.
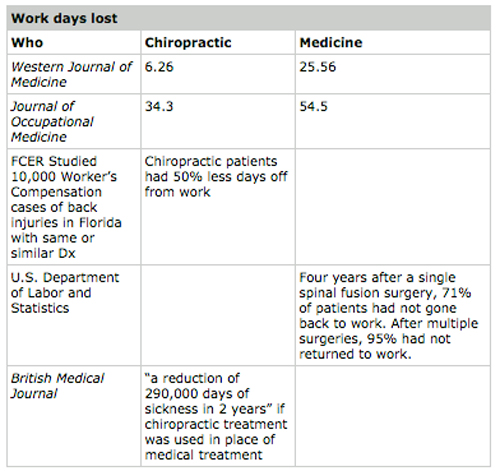
Treatment and Disability Costs: The Manga Report
A report for the government of Ontario, Canada, used to determine whether chiropractic should be included in their national healthcare program: “If chiropractors were the primary treating doctors for low back pain, there would be decreased hospitalization and disability and a ‘savings of hundreds of millions of dollars’. In fact, it is possible that chiropractors should be the ‘gatekeepers’ for lower back problems.”
Manga Report conclusions
- DCs are more effective for low back pain than MDs.
- No clinical or case control studies showed manipulation to be unsafe for LBP—in fact, it is far safer than medical Tx.
- If DCs were used, Canada would save hundreds of millions of dollars annually.
- Patients were more satisfied with chiropractic care.
- Despite medical disapproval and significant increased out of pocket expenses, chiropractic is growing.
- The Canadian Government should encourage people to shift to chiropractic treatment and consider making DCs the “gatekeepers” for low back pain.
Patient satisfaction
There have been dozens of studies on patient satisfaction regarding treatment by Medical Doctors, Doctors of Chiropractic, physical therapists, massage therapists, and mental health providers.
So far, every study comparing chiropractic care with medical care shows a significantly greater satisfaction with chiropractic. No study yet has shown otherwise.
AHCPR—U.S. Department of Health
- Acupuncture is not effective
- Physical therapy is not cost effective
- Only 1% of cases should receive surgery
- Epidural injections are rarely helpful and only in radicular involvement
- Antidepressant medication is not effective and can be dangerous
- Sclerosing injections are not effective
- Over the counter anti-inflammants are as effective as effective as prescription ones
- Shoe cushioning may be effective
- A few rest days followed by early movement and reintroduction into activity is important
- Manipulation is an effective treatment for low back pain
British Medical Journal
29% more patients improved under chiropractic care than those treated medically. This was measured during the three years after treatment, comparing pain, daily activities of living and satisfaction with their treatment. Chiropractic patients also expressed better sleep and were able to sit for longer periods.
Most significant fact
Average doctor of chiropractic’s annual malpractice costs: $4,134. Average medical doctor’s annual malpractice costs: $91,203. This speaks to how safe chiropractic is and how rarely chiropractors are sued.
The 2010 NBCE Review
The National Board of Chiropractic Examiners (NBCE) conducts a census-style survey of the profession every few years that helps ensure congruence between chiropractic practice and the educational curriculum.
The most recent survey, Practice Analysis of Chiropractic 2010, contains a chapter dedicated to a summary of current research.
This study, reprinted below with permission of Horace Elliot, current Executive Vice President of NBCE, is a valuable resource.
*Begin NBCE excerpt*
Chapter 2—Chiropractic Research
In the span of just 115 years since its inception, chiropractic has emerged as the third largest healthcare profession in the United States, offering diagnostic as well as therapeutic services to patients. It has reached the stature driven by research, which has made particularly significant strides over the past 30 years in spite of a budget that is a fraction of the dollars applied to medical and pharmaceutical research.
Like all health professions, chiropractic regularly tests the effectiveness, safety, patient satisfaction, and relative costs of its approach to healthcare. Basic science investigations, often using animal models, also help the profession to better understand the fundamental concepts of its methods. The results of these studies continue to show that chiropractors offer the public a unique and valuable form of health care, especially in the treatment of musculoskeletal problems such as back, neck, and headache pain. But chiropractic treatments are likewise proving, as documented to research, to be effective in the treatment of non-musculoskeletal health issues including infantile colic, enuresis, asthma, dysmenorrhea, otitis media, hypertension, and aberrations in heart rate variability. No other healthcare profession offers noninvasive solutions to such varied health concerns with equal safety and cost records.
After an extensive investigation, the Commission of Inquiry in New Zealand in 1979 was the first government panel to conclude that “modern chiropractic is a soundly-based and valuable branch of health care in a specialized area neglected by the medical profession” (Commission of Inquiry into Chiropractic, 1979). Over the ensuing 30 years, similar conclusions have been reached by government investigations in Australia (Thompson, 1996), Sweden Commission on Alternative Medicine, 1987), Canada (Manga, Angus, Papadopoulus, & Swan, 1993), Great Britain (Rosen, 1994), the United States (Bigos, Bowyer & Braen, 1994), and Denmark (Danish Institute for Health Technology Assessment, 1999). The research reported here demonstrates that chiropractic is becoming well-recognized as a patient-centered profession, informed by scientific evidence, and guided by clinical experience. In this chapter, we have focused our attention on investigations conducted in the past 10 years but have also included some earlier, important, and significant studies and literature reviews.
Effectiveness Research
For Back Pain
The most common reason patients seek chiropractic care is for back pain and disability (Christensen, Kollasch, Ward, & Webb, 2005). This topic, therefore, has received the most emphasis from chiropractic researchers. While there are many ways to investigate the effectiveness of the healthcare treatment, studies carried out in actual chiropractic practices, rather than in an artificial laboratory, are considered to have the greatest external validity, as they more accurately reflect actual conditions.
Practice-based Research
An important example of the use of practice-based research to investigate the effectiveness for low back problems was reported by Meade and colleagues (Meade, Dyer, Browne, & Frank, 1995; Meade, Dyer, Browne, Townsend, & Frank, 1990) I two studies. Meade et al. found that patients receiving chiropractic treatments reported pain and disability scores that were lower than those of the conventionally treated group by a clinically significant amount. A later study involving 2,870 patients with acute and chronic low back pain who visited either medical or chiropractic physicians’ offices yielded clinically important advantages in decreasing both pain and disability scores for those treated by chiropractors (Haas, Goldberg, & Attwood, 2004).
Dose-Response Studies
One area of investigation addresses important questions pertaining to two highly practical areas of chiropractic practice. First, how many treatments at what frequency will produce an optimal effect? Second, are the beneficial effects of spinal manipulation enhanced by including adjunctive therapies? Answers to these questions have been largely provided any recent study by Haas, Groupp, and Kramer (2004); they demonstrated that the beneficial effects of spinal manipulation for both pain and disability of the low back continue to accrue for up to 12 patient visits within a three week period (Hass et al., 2004). The implications were that, for at least some low back pain patients, cessation of treatments before 12 sessions are completed may be premature. The study also demonstrated that various physical modalities (electrotherapy, ultrasound, etc.) used in conjunction with spinal manipulation may achieve superior results. A longer-term study involving patients with chronic low back pain found that additional treatments every three weeks for nine months after completion of an initial 12 treatments in the first month conferred a distinct improvement in disability score (Descarreaux, Blouin, Drolet, Papadimitriou, & Teasdale, 2004).
Comparison with Other Treatments
It is always important that a proposed treatment be compared to other likely or common treatments for the same condition. One such study randomly allocated 115 patients with chronic back and neck pain to receive medication (nonsteroidal anti-inflammatory drugs), needle acupuncture, or chiropractic spinal manipulation. At the end of nine weeks of treatment (Giles & Muller, 2003) and also at the one-year follow-up (Muller & Giles, 2005), those who received chiropractic spinal manipulations displayed the best improvements in disability, range of motion, and pain scores. A similar study comparing patients receiving either vertebral manipulations or analgesic and/or anti-inflammatory medications demonstrated that pain and disability diminished in patients receiving the manipulations but not in those receiving medication (Elleuch & Ghouroubi, 2009).
Another recent study found that workers with back pain whose first visit to a healthcare provider was to a chiropractor were much less likely to be disabled at one year compared to workers who visited primary care physicians, occupational medicine specialists, or other medical specialists first (Turner et al., 2008).
Lumbar Disc Herniation
In a study that compared patients who received either conservative or surgical care for a herniated disc, the chiropractic patients were found to improve just as rapidly and completely in a randomized clinical trial (Weinstein, Tosteson, et al., 2006) and even more rapidly and completely when seen through the lens of an observational study (Weinstein, Lurie, et al., 2006). Two additional randomized trials that demonstrated the effectiveness of spinal manipulation compared to conventional treatments for lumbar disc herniation looked at range of motion changes in one group (Nwuga, 1982) and back pain, disability, and cost comparisons and another group of patients (Burton, Tillotson, & Cleary, 2000). Most recently, a randomized clinical trial found a substantial treatment effect for patients with acute back pain and sciatica with disc protrusion treated with spinal manipulation by chiropractors compared to a simulated manipulation (Santilli, Beghi, & Finucci, 2006).
Pediatric Low Back Pain
Regarding chiropractic treatment for low back pain in pediatric and adolescent populations, one cohort study (Hayden, Mior, & Verhoef, 2003) and three case studies (Hession & Donald, 1993; Kazemi, 1999; King, Mior, & Devonshire-Zielonka, 1996) involving spinal manipulation by a chiropractor have been reported. The cohort study revealed that 54 young patients receiving chiropractic care for back pain show distinct improvement in both a subjective scale and a pain questionnaire (Hayden et al., 2003). The three case studies describe the benefits of chiropractic treatment for adolescent patients with disc herniations associated with sports participation, including the return to all sports activities.
Systematic Reviews
There are now many studies documenting low back pain outcomes following chiropractic care (Meeker, Mootz, & Haldeman, 2002); many of these have been gathered into several comprehensive reviews for the scientific literature. An early milestone in this process was the RAND Corporation’s literature review of 67 articles and nine books published between 1952 and 1991. This review found that chiropractors performed 94% of all the manipulative care for which reimbursement was sought; osteopaths delivered 4% while general practitioners and orthopedic surgeons accounted for the remainder (Shekelle et al., 1991). A later appropriateness study by RAND presented a comprehensive array of over 1,500 clinical scenarios and rated this appropriateness of chiropractic intervention for each (Shekelle et al., 1991). The study served as the forerunner for many different types of studies, all of which provided substantial evidence in support of the chiropractic management of back pain
Early systematic reviews of randomized clinical trials emphasized acute rather than chronic low back pain as having the more robust evidence in support of manipulation’s effectiveness (Anderson et al., 1992; Bigos et al., 1994; Shekelle, Adams, Chassin, Hurzitz, & Brook, 1992). By 1997, however, evidence supporting the effectiveness of spinal manipulation compared to other interventions became more apparent for chronic conditions (Van Tulder, Koes, & Bouter, 1997). That trend has held up through the more contemporary, systematic reviews of Bronfort and colleagues (Bronfort, Haas, Evans, & Bouter, 2004; Bronfort, Haas, Evans, Kauchuk, & Dagenais, 2008) and very recently by the Scientific Commission of the Council on Chiropractic Guidelines and Practice Parameters (CCGP) (Lawrence et al., 2008). Recently, Chou and Hoffman (2007) performed a systematic review to help the American Pain Society and the American College of Physicians prepare a clinical practice guideline; they concluded that spinal manipulation was the most effective non-pharmacological treatment for acute and chronic low back pain.
For Neck Pain
Pain in the neck region is the second-most common reason people see chiropractic care (Christensen et al., 2005); thus, a number of studies have addressed pain in the neck region. A related topic that has also received attention from researchers is the difficulty in identifying and treating neck pain due to “whiplash-type” injuries.
Practice-based and Comparison Research
Several practice-based and comparison studies have found significant benefits in patients who received spinal manipulation as treatment for their neck pain. Koes et al. (1993) found that for subacute and chronic neck pain, improvements in the severity of the main complaint were larger with manipulative therapy than for physiotherapy. Cassidy and Hong-Hing (1992) reported that patients with unilateral neck pain and received spinal manipulation experienced a decrease in pain intensity that was more than 1.5 times greater than the comparison group who received mobilization. Rogers (1997) demonstrated improvements in pain and head repositioning that were 3–4 times greater in patients who receive manipulation than in the control group. In a randomized clinical trial, Hoving et al. (2002) found that the patients with neck pain who receive manual therapy reported market advantages over the groups given physical therapy or care by general practitioners. A second randomized trial revealed that patients who received spinal distraction manipulations in addition to electrotherapy reported significant improvements in pain, disability, and cervical motions (Gonzalez-Iglesia et al., 2009). Adding exercise regimens to manipulation by a chiropractor appears to confer additional benefits to neck pain patients (Gross et al., 2004).
Whiplash Disorder
“Whiplash” is a commonly used term for a neck injury received in motor vehicle collision. The problem facing both diagnosticians and victims of whiplash-associated disorders (WAD) is that in most moderate to severe cases are not detectable upon standard medical examination and are, therefore, difficult to define. Recent investigations have found that these injuries involve a broader array of soft tissue, neurological, and temporomandibular joint problems than presumed only a decade ago (Foreman & Croft, 1995). The result has produced controversy among healthcare professionals over the establishment of treatment guidelines (Freeman, Croft, & Rossignol, 1998: Spitzer, Skovron, & Salmi, 1995), even though chiropractic care appears to be beneficial. One study demonstrated that in subjects whose side bending of the neck was asymmetrical and who had a history of neck trauma, a single lower cervical adjustment delivered to the side of the most restricted movement was capable of reducing the extent of asymmetry for periods less than 48 hours (Nansel, Peneff, Cremate, & Carlson, 1990). Another investigation involving 93 patients in a retrospective review by structured telephone interviews found that those with restricted range of neck movement following whiplash injury were the most likely to improve after chiropractic manipulation (Khan, Cook, Gargan, & Bannister, 1999). Additional supporting evidence comes from a prospective study of 23 patients with subacute whiplash-associated disorders reported increased cervical range of motion and reduced pressure–pain threshold after cervical spine adjustments (Suter, Harris, Rosen, & Peterson, 2001).
Systematic Reviews
A special neck pain task force was recently commissioned by the Bone and Joint Decade (2000–10) to conduct a critical survey of the scientific literature published between 1980 and 2006. After extensive scholarly review, the task force recommended that most patients with neck pain would benefit from manual therapies (mobilization, manipulation, and massage), supervised exercises, low-level laser therapy, and perhaps acupuncture. Regaining function as soon as possible was considered to be a key component of those treatments found to be most effective (Hurwitz et al., 2008).
For Headaches
Published studies have generally classified headaches into several different groups; the most accepted classification system is recommended by the International Headache Society (IHS, 1988). The system now recognizes that pain in the head can be due to problems in the cervical spine. Chiropractic research pertaining to several types of headaches follows.
Tension and Cervicogenic Headaches
The leading study of the chiropractic treatment for tension-type headaches compared patients receiving chiropractic manipulation two others administered the antidepressant amitriptyline. Researchers found that during the four-week follow-up period, patients undergoing spinal manipulation maintained their improvements while medicated patients reverted to baseline (Boline, Kassak, Bronfort, & Anderson, 1995). A second randomized trial indicated that high-velocity thrusting compared to massage and trigger-point therapy did not confer additional benefits; however, both patient groups improved markedly over baseline values (Bove & Nilsson, 1998). Three other randomized trials supported the benefits of chiropractic treatment and management of tension headaches (Bitterli, Graf, Adler, & Mumenthaler, 1997; Hoyt et al., 1979; Vernon, 2009).
Cervicogenic headaches are similar to tension headaches are defined as pain originating in the cervical spine that is referred to the head (Bogduk, 1992; IHS, 1988). In comparing patients with cervicogenic headaches given either high-velocity cervical spinal manipulation or low-level laser treatments as a control, Nilsson, Christensen, and Harvigsen (1997) observed significant improvements of the manipulated group in terms of pain, headache hours per day, and use of medications. An additional clinical trial that compared patients receiving either nine upper cervical recoil adjustments or nine manipulations (simulated adjustments) demonstrated 28–36% reductions in headache frequency, duration, and severity, and also in medication consumption by those receiving adjustments (Whittingham, 2001). No such improvements were observed in the placebo group. Another randomized clinical trial by Jull et al. (2002) splits 200 cervicogenic headache participants into four groups receiving (1) a Maitland low- and high-velocity protocol for manipulative therapy. (2) a low-load endurance exercise regimen, (3) combined manipulative and exercise therapy, and (4) a control treatment. Each active intervention showed a significant reduction in headache frequency, intensity, duration, and neck pain compared to the control group (Jull et al., 2002).
Migraine and Vascular Headaches
Using a very similar design to the previous investigation of patients with tension headaches (comparing spinal manipulation to amytriptyline; Boline et al., 1995), Nelson et al. (1998) observed analogous results in their clinical trial involving patients with migraine headaches. This study added a group that received both amitriptyline and spinal manipulation for treatment, which did not result in any additional benefits. Clinically important improvements were initially seen in all these groups; however, significant differences emerged once again during the follow-up period with reductions of the headache index amounting to 24% for the amitriptyline group, 42% for spinal manipulation, and 25% for the group receiving combined treatments. By comparing manipulation to detuned ultrasound for treating migraine patients in another clinical trial, Tuchin, Pollard, and Bonello (2000) reported statistically significant improvements in headache frequency, duration, disability and medication use for patients receiving spinal manipulation. In their study of patients with unclassified post-traumatic headaches, Jensen, Nielsen and Vosmar (1990) compared cold packs with mobilization in a third clinical trial and demonstrated a reduction of pain by 43% in the manual therapy population compared to the cold therapy group at two weeks following treatment.
Pediatric Headaches
While there have been no formally constructed outcome trials of manipulation in pediatric populations with headaches, there are numerous case studies and case series, some of which have appeared in peer-reviewed journals. Successful treatment of tension type, cervicogenic, and even migraine headaches in children have been described (Hewitt, 1994).
Systematic Reviews
To verify the clinical outcomes’ evidence supporting spinal manipulation and various other physical and behavioral interventions in the management of headaches, the Agency for Health Quality and Research began a systematic literature review. The eventual result was an evidence report from the Duke Center for Health Policy Research and Education (McCrory, Penzien, Hassselblad, & Gray, 2001) which concluded that non-pharmacological treatments are of growing importance and, “if effective and available… [they] may be the first choice for most patients” (p.11). Furthermore, the report indicated that drug treatments are not suitable for all patients, may produce undesired side effects, and are not universally effective.
For the Extremities
Over the past decade, the extremities have become increasingly recognized as an area responsive to manual therapy; moreover, reports indicate that upper and lower extremity problems account for about 20% of all chiropractic care (Cherkin et al., 2002; Christensen et al., 2005; Mootz et al., 2005). For instance, a clinical trial concerning the shoulder girdle that compared usual medical care both with and without high-velocity low-amplitude manipulations revealed that spinal manipulation accelerated the recovery from shoulder symptoms (Bergman, et al., 2004). Regarding carpal tunnel syndrome, a clinical trial (Winters, Sobel, Gronier, Arendzen, & Meyboom-de-Jong, 1997) and another investigation (Strait & Kuchera, 1994) demonstrated that manipulative therapy have the potential to speed the rate of improvement in patients with this condition.
Two extensive literature reviews addressing chiropractic treatment of the lower extremities have recently been published (Brantingham, et al., 2009; Hoskins, McHardy, Pollard, Windsham, & Onley, 2006). In spite of the lack of controlled research studies, these reviews reported that there was considerable case evidence supporting the use of manipulative therapy for knee osteoarthritis, but hello for all pain syndrome, and ankle inversion sprain, and perhaps for hip osteoarthritis.
For Non-musculoskeletal Conditions
An early indication that non-musculoskeletal as well as musculoskeletal conditions were responsive to chiropractic care came from a study conducted by 87 members of the Swedish Chiropractic Association; each association members surveyed 20 consecutive adult patients who had initiated care for a musculoskeletal complaint. They found that 23% of their patients reported at least one positive benefit extended beyond the musculoskeletal system; the most commonly reported improvements involved respiratory and digestive systems (Lebouef-Yde et al., 1999). An international research consortium’s survey of 5,607 patients from seven countries later confirmed these results (Lebouef-Yde et al., 2005).
Infant colic, bed-wetting, ear inflammation, and asthma
To buttress years of promising clinical observations that found chiropractic treatments helpful in reducing or eliminating colic in infants, several studies have recently been conducted (Olafsdottier, Forshei, Fluge, & Markestad, 2001; Wilberg, Nordsteen, & Nilsson, 1999). The results from treatment of more than 450 infants were generally positive. These studies involved chiropractic spinal manipulation applied either by fingertip or with a computer-assisted adjusting device.
Clinical studies that included over 200 patients (Reed, Beavers, Reddy, & Kern, 1994) suggest that spinal manipulative therapy may play a role in helping to manage bed-wetting (enuresis). The positive results of one randomized clinical trial in particular (rReed et al., 1994) are difficult to ignore.
Otitis media is the term used to describe inflammation of the middle ear—the region behind the eardrum. Although randomized clinical trials have yet to be performed, large cohort and case studies of more than 850 young patients provide support for the effectiveness of chiropractic or osteopathic manipulative therapy for this condition (Froehle, 1996). The majority of otitis media cases treated with spinal manipulation appeared to resolve within 10 days; most responded to fewer than five adjustments and many required only one or two treatments (Fallon, 1997).
In addition to case studies that have reported positive clinical effects of spinal manipulation for asthma (Beyeler, 1956), four randomized clinical trials, three cohort studies, one crossover investigation, and four case studies involving over 550 patients offer measurable support for spinal manipulative therapy in the management of this condition (Ali, Hayek, Holland, McKelvey, & Boyce, 2002; Balon et al., 1998). Lung function improvements may not be detectable (Balon et al., 1998; Bronfort, Evans, Kubic, & Filkin, 2002) but quality of life scores improved by 10–28%, led by activity scale changes (Kokjohn, Schmid, Triano, & Brennan, 1992). The largest randomized clinical trial to date that is attempting to compare several different manipulative techniques in the management of asthma is currently underway in Australia. Although data on symptoms, quality of life, and distress are forthcoming in the study, preliminary measurements show that a stress hormone (cortisol) decreases with manipulation compared to patients who visit healthcare providers but do not receive treatment (Ali, et al., 2002).
Painful Menses, High Blood Pressure, and Heart Rate Variability
Outcome studies of chiropractic care of more than 250 patients experiencing dysmenorrhea and premenstrual syndrome found marked improvements and menstrual pain and distress (Hondras & Brennan, 1999; Kokjohn et al., 1992; Walsh & Polus, 1999). Particularly noteworthy are the results from a pilot study performed by Kokjohn et al. that revealed noticeable improvements for patients subjected to manipulative forces in a side-posture procedure. It was evident that such patients experienced reductions in pain and improvements in their menstrual distress survey scores as well as significant decreases in the levels of hormones (prostaglandins) associated with menstrual cramping. This investigation identified positive clinical outcomes as well as likely physiological mechanism that clearly resulted from the chiropractic intervention (Kokjohn et al., 1992).
The effects of chiropractic care on patients with high blood pressure have been reported from two each of the following: randomized clinical trials, pilot studies, crossover designs, nonequivalent comparisons, case series, case studies, and one cohort study. While the specific results varied, they often revealed significant decreases in blood pressure (Plaugher et al., 2002; Yates, Lamping, Abram, & Wright, 1988). One of the most dramatic decreases in both systolic and diastolic pressure (13mm and 8mm, respectively, at week 8) has recently been reported by Bakris et al. (2007) in a study of low-force chiropractic intervention applied to the upper neck region.
Improvement in the variability of the heart’s rate of beating following spinal manipulation has been demonstrated in 60 patients, primarily in studies using crossover randomized clinical trials. Increases of frequency ranges (indicative of greater sympathetic output to the heart) were reported by Budgell and Hirano (2001) following either upper cervical or thoracic manipulations (Budgell & Polus, 2006). Welch and Boone (2008) reported a similar result in three patients who received spinal manipulation in the thoracic region but described a decrease in frequencies (indicating a relativeincrease in parasympathetic activity) after manipulations in the cervical region. While the opposing effects of manipulation the sympathetic in parasympathetic nervous system activity appear to be linked to manipulation in different regions of the spine, this particular finding needs to be repeated with a substantially larger population of patients.
Central Nervous System Function
Spinal manipulation may change the way the central nervous system processes messages. These apparent alterations affect both somatosensory transmission (Zhu, Haldeman, Starr, Seffinger, & Su, 1993) and motor control (Hodges & Rochardson, 1996). Improvements in cognitive processing to support this model have been shown in a prospective double-blind, randomized trial (Kelly, Murphy, & Backhouse, 2000) and in a cohort study comparing manipulated to nonmanipulated groups (Smith, Dainoff, & Smith, 2006).
Systematic Reviews
A systematic review of the scientific literature identified 179 published papers that addressed chiropractic care for 50 different non-musculoskeletal conditions. While the majority of these were case studies or case series, 47 papers describe experimental studies including 14 randomized trials. Based on their review of the controlled studies, the authors determined that there was evidence of benefit of chiropractic care for patients with asthma, cervicogenic vertigo, and infantile colic, and potential benefit for children with otitis media and elderly patients with pneumonia (Hawk, Khorsan, Lisi, Ferrance, & Evans, 2007).
For Prevention and Wellness
Chiropractic’s role in prevention has been demonstrated in a comparative study performed by the RAND Corporation. Elderly patients under continuing chiropractic care were more likely than patients not receiving such care to be free of hospitalizations or the use of a nursing home, more likely to report a better health status, and more likely to be mobile in the community (Coulter, Hurwitz, Aronow, Cassata, & Beck, 1996). Another study found that treatment of patients with manual therapy, exercise, and biopsychosocial education conferred superior disability, mood, general health, and quality of life scores in comparison to patients with no treatment (Wand et al., 2004). Meeker and Haldeman (2002) reported that a significant number of patients use chiropractic care to enhance their well-being and quality of life.
An on-site industrial chiropractic program resulted in significant reductions in days of lost time, costs per claim, rate premiums, and the number of surgeries (Cooper & Pfefer, 2007). Importantly, another study involving two elite Australian Rules football teams who were randomly assigned to two groups (one receiving a chiropractic management program in addition to the standard therapies given to both groups) revealed that the chiropractic intervention resulted in fewer injuries to the hamstrings, lower limb muscles, and knees (Hoskins & Pollard, 2007).
But perhaps the most compelling data of all comes from a study (Descarreaux et al., 2004) of patients with chronic low back pain who were randomly assigned to one of two groups. One received a chiropractic adjustment every three weeks beyond the 12 treatments given within the first month to both groups. The group receiving the supplementary maintenance treatments continued to display reductions in disability, while the cohort lacking the additional visits reverted to baseline levels.
Safety and Satisfaction Research
A Safe Intervention
All treatments must be assessed for the frequency and severity of any adverse effects. Chiropractic treatments have been found to be quite safe with minimal risk of primarily minor adverse effects. One large review of English language medical literature for the period from 1926 to 1993 found a total of 128 articles that reported 185 specific complications attributed to manipulation of the cervical, thoracic, or lumbar spinal regions. Vick, McKay, and Znegarle (1996) concluded:
Of the estimated several hundred million manipulative treatments performed each year, only 185 reports of injury were found in the published literature in the past 68 years. Comparing these figures with the incidence of adverse effects (including death) associated with many pharmaceutical agents, manipulative treatment remains an extremely safe therapeutic modality when performed by knowledgeable and skilled practitioner (p. 114).
A second study retrieving numerous case studies, case-control, retrospective and prospective studies, surveys and a randomized controlled trial from 1966–2007 indicated that most adverse events could be attributed to spinal manipulation were benign and transitory; however, the data were deemed insufficient to assess their actual prevalence in the general population (Gouvela, Castanho, & Ferreira, 2009).
Side Effects and Risks
The most common adverse effects of chiropractic treatment are short-term soreness and/or a temporary increase in pain. The likelihood of initial soreness or increase pain has been found to be similar to that of starting an exercise program (Bronfort et al., 2001; Hurwitz, Morgenstern, Vassilaki, & Chiang, 2005).
While some reports suggest that spinal manipulation is capable of causing disc herniations and cauda equina syndrome (Assendelft, Bouter, & Knipschild, 1996), the risk is low, with estimates of the frequency of such events arising from spinal manipulations ranging from 1 in 1 million (Assendelft et al., 1996; Patijn, 1991) to 1 in over 100 million (Shekelle et al., 1992). When a condition occurs that rarely, it is very difficult to determine which of many prior factors was the actual cause.
Cerebrovascular Accidents
The most serious adverse event that may occur in conjunction with chiropractic manipulation is a stroke associated with the vertebral artery dissection (VAD; Rothwell, Bondy, & Williams, 2001; Smith et al., 2003). This uncommon occurrence (also called the cerebrovascular accident or CPA) is caused by internal bleeding of the artery that supplies the brain. Several retrospective studies investigating large population bases have been conducted to identify and quantify the risks of cervical manipulation and producing ZADs. These studies indicate that the number of serious complications or cerebrovascular accidents (established by researchers from both the chiropractic and medical professions) ranges from 1 case per 400,000 manipulations (Dvorak & Orelli, 1985) to zero in 5,000,000 (Jaskoviak, 1980). A more recent retrospective review of malpractice claims from the Canadian Chiropractic Protective Association found a frequency rate of one per 5.85 million (0.17 per million) cervical manipulations (Haldeman, Carey, Townsend, & Papadopoulos, 2001). The risk estimates attributed to cervical manipulation are significantly less (by orders of magnitude) than those associated with various medical procedures and even simple lifestyle activities (Dabbs & Lauretti, 1995; Dinman, 1980).
Perhaps the most important concept that needs to be understood is the fact that a significant number, and most likely the majority of VADs, happened to be spontaneous vertebral artery dissections (sVADs). The annual incidence of sVADs in hospital settings has been estimated to occur at the rate of 1–1.5 per 100,000 patients (Shievink, Mokri, & O’Fallon, 1994) and in community settings to be twice as high (Shievink, Mokri, & Whisnat, 1993). In a recent study of 818 VAD strokes in a hospitalized population of over 100 million person-years, Cassidy et al. (2008) demonstrated that the association of strokes and visits to either chiropractors were primary care physicians was equal, suggesting that the cause of strokes could not be associated with any element unique to chiropractic care. More likely the strokes were already in progress and causing symptoms that prompted the patients to seek healthcare intervention.
Dabbs and Lauretti (1995) compared the risk of serious complication or death for patients with neck pain who received either manipulative treatment or nonsteroidal anti-inflammatory drugs (NSAIDs). They concluded, “Therefore, based on the best available evidence, we calculate the risk of serious complications or death is 100-400 times greater for the use of NSAIDs than for the use of cervical manipulation in the treatment of similar conditions” (p. 534).
Patient Satisfaction Studies
Research in the vital area of patient satisfaction finds that doctors of chiropractic consistently received high marks from their patients. Chiropractic management of spine disorders is often more successful the medical treatment; this results in higher levels of patient satisfaction. In a comparison study between doctors of chiropractic and medical practitioners, Nyiendo, Haas, and Goodwin (2000) found, “Patients with chronic low back pain treated by chiropractors show greater improvement and satisfaction at 1 month than patients treated by family physicians. Satisfaction scores were higher for chiropractic patients” (p.239). A higher proportion of chiropractic patients in the study (56% vs. 13%) reported that their low back pain was better or much better, whereas more than one-third of medical patients reported their pain was worse or much worse (35% vs. only 14% for patients of chiropractors).
There is a growing body of research that documents patient satisfaction with the manner, care, and explanations of treatment by doctors of chiropractic (Coulter et al., 2003; Gemmell & Hayes, 2001; Hawk, Long, & Boulanger, 2001). The final report to the Department of Defense from its Chiropractic Healthcare Demonstration Project found that participants who received chiropractic care strongly agree that they had good treatment results. They expressed more satisfaction with a chiropractor’s willingness to spend time with them, with explanations of treatments, and with health condition improvements compared to those who received medical care Birch & Davis Associates, 2000). A survey of Canadian military personnel who were involved in a similar demonstration study investigating the inclusion of chiropractic care reported that “the majority of military personnel (94.2%) and referring physicians (80.0%) expressed satisfaction with chiropractic services” (Boudreau, Busse, & McBride, 2006, p. 574).
More recently, the final report of the Medicare Demonstration Project that was conducted from April 2005 to March 2007 found:
Satisfaction with (chiropractic) care was high, with 87% reporting levels of 8 or higher on a 10-point scale and 56% indicating a perfect score of 10. Sixty percent of respondents indicated that was the received “moderate” or “complete” relief from chiropractic treatments compared to 11% from treatments by other health professionals (Stason et al., 2010, p. 7).
Cost-Effectiveness Research
Given that rising healthcare costs and American now consumes 16% of the Gross National Product and that their inflation of nearly 8% in 2004 was almost triple the overall national inflation rate (Smith, Cowan, Sensenig, Catlin, & Team, 2006), cost-effectiveness is clearly a major factor in assessing appropriate health services. As the sixth most expensive health condition in the United States the cost of spine pain was 86 billion dollars in 2005, an increase of 65% since 1997 (Martin, et al., 2008). Studying the cost-effectiveness of any health service is difficult due to the variation in patient characteristics, payment incentives, and the proprietary and fragmented nature of most billing records. Some of the clearest data have come from studies of work injuries, as discussed below. There now have been several attempts by economists to evaluate the cost-effectiveness of chiropractic care.
Workers Compensation Data
When chiropractic costs were compared to care for medical providers or physical therapists, considerable savings were found with the use of chiropractic care in Florida (Folsom & Holloway, 2002), Texas (MGT of America, 2003), North Carolina (Phelan, Armstrong, Knox, Hubka, and Ainbinder, 2004), and Oklahoma (MGT, 2005).
Similar data were obtained from workers’ compensation records obtained in Australia (Ebrall, 1992). Because laws and regulations regarding workers compensation vary considerably among states and regions, firm general conclusions are difficult to ascertain. However it appears that chiropractors are underutilized in many workers’ compensation systems. According to records of disbursements to medical and chiropractic physicians and physical therapists in the state of Georgia from 2006-2009 for back pain in workers’ compensation cases, chiropractors received 2% or less of the funds paid to medical physicians and just 1.4–11.7% of the disbursements paid to physical therapists (Georgia.gov, n.d., State Board of Workers’ Compensation, “Statistics”).
Insurance Company Data
Insurance companies often use larger databases that are less prone to potential skewing by regional variations in workers’ compensation laws. All retrospective studies of claims data, however, have to deal with the difficulty of verifying that the computerized data correspond to the actual conditions experienced in the treatments rendered.
Several early studies from Utah (Jarvis, Phillips, & Morris, 1991), Iowa (Johnson, 1989), and Florida (Wolk, 1988) provided data that suggested a significant savings in costs when chiropractic care was compared to medical care for back problems. The work of Stano and Smith (1996), who also demonstrated significant cost savings for chiropractic care, provided a key conceptual advance by carefully defining episodes of treatment in addition to including all relevant treatment costs. More recent data have suggested that, although chiropractic costs sometimes appear to be higher, these elevations are more than offset by the clinically important differences in pain and disability improvement found only in the chiropractic patients ( Haas, Sharma, & Stano, 2005).
Sarnat, Winterstein, and Cambron (2007) found that admitting chiropractors into a health-care plan as gatekeepers led to dramatic cost reductions, exemplified by 59% fewer hospital days, 62% fewer outpatient surgeries, an 83% lower pharmaceutical costs. Including a chiropractic benefit in a managed-care plan resulted in lower annual total healthcare expenditures, even though all pharmacy, physical therapy, and post-surgical costs were emitted from the itemized expenditures for medical care (Legoretta et al., 2004). The results of a study within the frame work of Medicare indicated that chiropractic care significantly reduces per beneficiary cost of the program (Muse and Associates, 2001). A large analysis of 4 years of claims data from a managed care health plan found that patients who had access to chiropractic care had fewer neuromusculoskeletal complaints than those without access; that chiropractic care was a direct substitution for medical care, not an additional cost (Metz, Nelson, LaBrot, & Pelletier, 2004). This group also had a significant reduction in the use of high-cost and invasive procedures for treatment of low back and neck pain (Nelson, Metz, & LaBrot, 2005).
Economist Evaluations
Pran Manga, an economist at the University of Ottawa, was commissioned twice by the Provincial Government of Ontario to assess the effectiveness and cost-effectiveness of chiropractic management of low back pain. His assessment of the comparative cost data in his first report led him to conclude the following:
There is an overwhelming body of evidence indicating that chiropractic management of low back pain is more cost-effective than medical management. We reviewed numerous studies that range from very persuasive to convincing in support of this conclusion. The lack of any convincing argument or evidence to the contrary must be noted and is significant to us in forming our conclusions and recommendations (Manga et al., 1993, p. 11).
In his second report, Manga (1998) found the cost advantages for chiropractic care of matched conditions to be so dramatic that he concluded that “doubling the utilization of chiropractic services from 10% to 20% may realize savings as much as $700 million in direct costs and $3.8 billion in indirect costs” (p. 1).
A more recent evaluation of the cost-effectiveness of chiropractic care, the Mercer Report, came to the following conclusions (Choudry & Milstein, 2009):
- Chiropractic care is more effective than other modalities for treating low back pain and neck pain.
- For low back pain, chiropractic physician careincreases total annual per patient spending by $75 compared to medical physician care.
- For neck pain, chiropractic physician care reducestotal annual per patient spending by $302 compared to medical physician care.
- When considering effectiveness and cost together, chiropractic physician care for low back and neck pain is highly cost-effective, [and] represents a good value in comparison to medical physician care and to widely accepted cost-effectiveness thresholds.
These researchers admitted that, because they were unable to capture and incorporate the cost of any prescribed drugs, their estimate of the comparative cost-effectiveness of chiropractic care was likely to be understated.
Basic Science Research
Investigation of the chiropractic approach to health care has also studied animal models. The key reasons for using a test organism in research are that it prevents a simplified picture of an area of interest and lends itself to experimental situations that are difficult or impossible to perform with human subjects. Another prominent feature and advantage to the test organism is it allows direct examination of living tissues, shedding further light upon complex biological interactions. Some examples of chiropractic basic research that used animal models are listed below.
Anatomy and Biomechanics
One of the most inclusive animal models of subluxation and the application of biomechanics has come from the novel external fixation model in rats developed by Henderson, Cramer and coworkers at both the National University of Health Sciences and Palmer University (Henderson, Cramer, Zhang, DeVocht, & Fournier, 2007). The spinous processes of rats’ vertebra from L4 to L6 were fixated using a noninvasive, removable yoke for up to eight weeks. Osteophytes and degenerative articular changes of the facet joints could be observed for fixation times as short as one week and became irreversible after four weeks of fixation (Cramer, Fourner, Henderson, & Wolcott, 2004). In addition, increases in synapse density were identified, indicating significant changes to the nerves in the fixated region (Bakkum, Henderson, Hong & Cramer, 2007). These studies begin to shed light on the significant effects of fixation and hypomobility.
Chiropractic theory suggests that an essential component of the vertebral subluxation complex is the development of adhesions and the zygopophyseal joints as a result of hypomobility that develops in these structures (Janse, 1976; Mooney & Robertsen, 1976); spinal manipulation is capable of breaking up these fixations in a process known as “gapping” (Engel & Bogduk, 1982; Giles & Taylor, 1987). The finding by Cramer and his colleagues that gapping did indeed occur in healthy volunteers subjected to spinal manipulation (Cramer et al., 2000, 2002) provided noteworthy support to this aspect of chiropractic theory and practice.
Neurology
A wide variety of neurological studies are simply not possible to perform in humans; thus, animal models have been quite helpful for providing additional evidence for the neurological aspects of chiropractic theory by studying the response to various types of interventions, all involving noxious stimuli (Araki, Ito, Kurosawa, & 1981; Brennan et al., 1991; Christensen, Beals, Burnham, Magnani, &; Urbanek, 1991; Christiansen& Meyer, 1987; DeBoer, Schutz, & McKnight, 1988; Gillette, Kramis, & Roberts, 1993; Hu, Yu, Vernon, & Sessle, 1993; Israel, 1983; Sato & Sato, 1985; Sato & Swenson, 1984; Triano & Luttges, 1980).
Investigations using rats have been able to elicit decreases in both mean arterial pressure and nerve blood flow following saline injections into the ipsilateral L4/L5 facet joint (Budgell, Holtz, & Sato, 1995). Previous experiments by Sato, Sato, Shimado, and Torigata (1975) demonstrated decreased gastric motility in response to a somatic stimulation (skin pinch). These experiments support some of chiropractic’s concepts of the linkage between spinal aberrations and more generalized physiological disturbances including the functioning of the viscera. Insertion of a small pan into the intervertebral foramen of the L4 and L5 vertebral joints of the experimental rat, mimicking a space-reducing lesion, produce thermal and mechanical hyperalgesia in the hind limb and increase the excitability of dorsal root ganglion cells (Song, Vizcarra, Xu, Rupert, & Wong, 2003; Song, Xu, Vizcarra, & Rupert, 2003). The same responses were observed within the injection of an inflammatory cocktail into the same region (Song, Gan, Cao, Wang, & Rupert, 2006). Elsewhere, it has been shown that there may be interaction between the stimulation of spinal joint receptors and the processing mechanisms for spinal reflexes. Specifically, when spinal joint receptors in the rat were activated, reflex responses in the paraspinal muscles were diminished (Indahl, Kaigle, Reikeras, & Holm, 1997).
In an experiment using cats, the muscle spindles and Golgi tendon organs in paraspinal muscles were seen to respond to vertebral loads with force-time profiles resembling those in spinal manipulation (Pickar & Wheeler, 2001). That these proprioceptors displayed a unique response to the thrusting portion of the applied load suggests that the receptors may contribute to the therapeutic effects of spinal manipulation (Dishman & Bubulian, 2000).
Hormones and Inflammation
A considerable body of research has demonstrated that—through a complex system of feedback loops and interactions—a close communication among the central nervous system, the immune system, and various hormones by means of the hypothalamic-pituitary-adrenal (HPA) axis exists (Bassett, Marshall, & Spillane, 1987). Both chronic stress and acute inflammation can disrupt the normal balance of hormones and lead to immune system malfunction. Of special interest is that control of the inflammatory process can be linked directly to manipulation; preliminary evidence in both animal models and humans suggests that spinal manipulation may be effective in retarding or reducing several indicators of inflammation. Included are thermal and mechanical sensitivity, neurophysiologic reactivity, cellular inflammation, and blood serum levels of the pro-inflammatory cytokines tumor necrosis factor alpha and IL-6 (Teodorczyk-Injeyan, Injeyan, & Ruegg, 2006, 2007). By injecting inflammatory cocktail directly into the L5 intervertebral foramen of experimental rats, Song and his colleagues (2006) were able to evoke a broad spectrum of indicators of neural excitability and inflammation including thermal hyperalgesia (hypersensitivity to heat), allodynia (hypersensitivity to a non-noxious stimulus), hyperexcitability of the dorsal root ganglia on electrical recordings, and visual evidence of cellular inflammation seen under the microscope. All these indicators decreased following the application of mechanical manipulations to the L5 or L5 and L6 spinous processes by means of an adjusting instrument; no such effects were seen in the manipulation was directed to the L4 joint. The implication was that mechanically applied manipulation can significantly reduce the severity and duration of pain and hyperlgesia caused by irritation at the lumbar intervertebral foramen (Song et al., 2006).
Conclusions
Today, the chiropractic approach to health care is supported by a wide variety of research—from practice-based studies to cost-effectiveness comparisons to basic science investigations in animals. While there is still an ongoing debate regarding the best practices and optimal treatment protocols, the current evidence is overwhelming that doctors of chiropractic provide an important and necessary health care service at a reasonable cost. The risks of spinal manipulation, while remaining an objective for further research, are considerably less than those encountered for medical interventions treating the same or similar conditions. In concert with current efforts to emphasize prevention and the maintenance of good health and to reap significant monetary savings in the process, chiropractic management has been found to forestall and/or prevent further health concerns, disabilities, and expenses. As a result, the chiropractic profession continues to gain ever broadening acceptance and support from patients, payers, and healthcare decision-makers.
*End NBCE excerpt*
Direct Links
Below, organized by topic, are external links to published studies, abstracts, or media reports on studies not published online.
Cost effectiveness: paid costs for episodes of care initiated with a DC are almost 40% less than episodes initiated with an MD
Liliedahl RL, Finch MD, Axene DV, Goertz CM. Cost of Care for Common Back Pain Conditions Initiated With Chiropractic Doctor vs Medical Doctor/Doctor of Osteopathy as First Physician: Experience of One Tennessee-Based General Health Insurer. Journal of Manipulative Physiological Therapeutics. November–December 2010;33(9):640–43.
Chiropractic and Economic Cost Effectiveness 2010
Chiropractic results in a reduction in the rates of surgery, advanced imaging, inpatient care, and plain-film radiographs
Nelson CF, Metz RD, LaBrot T. Effects of a managed chiropractic benefit on the use of specific diagnostic and therapeutic procedures in the treatment of low back and neck pain. Journal of Manipulative Physiological Therapeutics. Oct 2005;28(8):564–69.
Hundreds of cases of decades-long chronic headaches respond to upper cervical adjusting
Upper cervical chiropractic care for a patient with chronic migraine headaches with an appendix summarizing an additional 100 headache cases.Erin L. Elster, DC. Journal of Vertebral Subluxation Research. August 3, 2003.
Chiropractic care shows symptomatic improvements in autism-related behaviors following treatment
Autism, a Chiropractic Perspective. Jane Jennings and Martina Barker. Clinical Chiropractic. March 2006. 9(1): 6–10.
The relationship between chiropractic care and psychological and emotional health and disease
Body, Mind and Chiropractic. Christopher Kent, DC, Esq. Dynamic Chiropractic. June 17, 2010, Vol. 28, Issue 13.
Chiropractic improves attention in adults, maybe by creating plastic changes in the prefrontal cortex and other cortical and subcortical areas
Improvement in Attention in Patients Undergoing Network Spinal Analysis: A Case Series Using Objective Measures of Attention. Yannick Pauli, DC.Journal of Vertebral Subluxation Research. August 23, 2007, pp 1–9.
Preliminary studies suggest a positive effect of chiropractic care in individuals suffering from learning disabilities and dyslexia
The Effects of Chiropractic Care on Individuals Suffering from Learning Disabilities and Dyslexia: A Review of the Literature. Yannick Pauli, DC. Journal of Vertebral Subluxation Research. January 15, 2007, pp 1–12.
Chiropractic most effective (for neck, low back, headache, acute and chronic pain), most cost-effective and most liked form of health care
Excerpt from Liliedahl et al (2010). Journal of Manipulative and Physiological Therapeutics.
Chiropractic care effective for major, long-term depression
Effect of Subluxation-Based Chiropractic Care on Quality of Life in a Patient With Major Depression. Alain M.J. Desaulniers. Journal of Vertebral Subluxation Research.April 23, 2008.
Chiropractic Care Eases Severe Depression
Copyright 2005-2017 Centre Chiropractic, PC
Copyright 2010 NBCE, used by permission
Get our free newsletter, Centred on Health
![]() We'll never sell or share your information
We'll never sell or share your information
